KSA Value Based Healthcare – Developments in implementation in 2024
Healthcare & Life Sciences Focus
Christina SochackiSenior Counsel,Corporate Commercial
Under Vision 2030, KSA examined its healthcare sector and saw a number of significant challenges; the result has been an increasing healthcare budget and investment into the sector, including significant reform, following both regional and global trends. For example, as part of Vision 2030 and the Ministry of Health’s (‘MOH’) Healthcare Transformation Strategy, the MOH is migrating all existing MOH providers into healthcare clusters, which will be geographically defined, vertically integrated, “Accountable Care Organisations” across the Kingdom. The goals of decentralisation and clustering public health service delivery is to increase competition, transparency, and efficiency as health clusters compete with each other as well as the private sector for clients and health care professionals.
As the Kingdom seeks to shift to the "new model of care", delivered through its network of health clusters being formed, the MOH issued the first edition of the Health Cluster Management Guide, 2024, which includes several standards and requirements to ensure that health facilities affiliated with the MOH apply the best health practices and standards as applicable to the capabilities of the public sector facilities.
On the other hand, as part of its new vision and strategy, the Council of Health Insurance (‘CHI’) plans a transformation journey from today’s volume driven scheme (with misaligned incentives), towards a value-based health system (with value at the center and aligned incentives); below we explore its new value-based healthcare action plan.
Oversight of these health standards in a transparent way will be crucial to achieving success and sustainability, ensuring policies and procedures are implemented correctly, and limiting risks and abuses. The guide includes a variety of checklist type standards for an assortment of care settings and departments, including those in:
hospitals;
home healthcare;
long term care and medical rehabilitation;
primary health care centers;
laboratories;
blood banks; and
forensic services centers.
It also includes cybersecurity standards as well as standards for engineering services, maintenance, and operation. Finally, the second chapter addresses the technical and administrative staff as well as healthcare practitioners.
The Council of Health Insurance (‘CHI’) launched a new Action Plan aims to disseminate and explain the vision and plans for Value-Based Health Care (‘VBHC’) in the Kingdom of Saudi Arabia.
Most of the programs that are part of CHI's 2020-2024 strategy contribute to the VBHC agenda. For example: the value-based payment initiatives; implementation of NPHIES and data standards; payer and provider benchmarking; and casemix and patient classification systems (DRGs in this case).
As part of this new strategy, CHI has devised the following strategic objectives:
Enable target population segments to be fully covered and protected;
Operate as a reliable, lean, and learning regulator;
Improve the sustainability and innovation of the sector;
Catalyze the digital transformation of the sector; and
Enable payers and providers to improve their services to beneficiaries with progressive policies.
Current State:Currently, the CHI scheme for the private sector is very transactional, with large volumes of itemized and packaged claims submissions, adjudication, and payment for rendered services. Annually, CHI reports that there are around 80 million claims (with a value of almost SAR 25 billion), adjudicated through payments entirely based on a fee-for-service (‘FFS’) model and with none or limited outcome or performance related payments.
As such, as a volume driven health system, consensus is that it is prone to higher risks of supplier-induced demand and increased levels of fraud, waste, and abuse. In addition, volumes of better care are not correlated with better outcomes and health, and these could also represent a waste to the system.
VBHC VisionAs part of its new vision and strategy, CHI plans a transformation journey from today’s volume driven scheme (with misaligned incentives), towards a value-based health system (with value at the center and aligned incentives), through three main strategic objective aims:
Designing healthcare around the beneficiary;To this end, the CHI has created the National Patient Reported Outcome Measure (‘NPROM’) strategy. CHI has taken the initiative to create a strategy to standardize the way they gather and improve the quality of the Patient Reported Measures (‘PRMs’). PRMs (i.e., any report of the status of a patient’s health condition, health behavior, or experience with healthcare that comes directly from the patient, without interpretation of the patient’s response by a clinician or anyone else) are a means of assessing and improving the quality of care, and aree now becoming a widely used tool in developed countries. These developments have led to distinguishing Patient Reported Outcome Measures (‘PROM’) and Patient Reported Experience Measures (‘PREM’).
Improving health outcomes for the beneficiariesThe goal of the project is to build the CHI Population Health Management (‘PHM’) program in line with national requirements and best practices. To achieve that, the project includes two workstreams 1) Population Health Management Program, which will include developing a PHM guide; and 2) Population Health Data and Analytics, which will include defining KPIs to support performance measurement, build dynamic dashboards, as well as develop a PHM use cases.
CHI developed a list of primary care initiatives, including one to design and implement a pilot specifically for the classification framework initiative across six pilot sites. This entails developing a classification framework with criteria that specify the minimum requirements of a robust primary care service, and also includes defining a list of primary care measures to measure the quality of services and outcomes of primary care and to ensure continuous improvement and excellence.
The last part of the project will be to develop a scale up plan where CHI will outline a detailed plan with future recommendations for the scaling up of the classification system to additional sites across the Kingdom.
Developing innovative financing models - paying for qualityThe Council plans to introduce a combination of different models of payments for healthcare services. While the plan is to shift from FFS to VBHC, it is not expected that FFS will be completely replaced, given that some services by their nature can only be paid based on a FFS model. Nevertheless, CHI is considering introducing performance-based modification of FFS where applicable and necessary (i.e. Pay for Performance models).
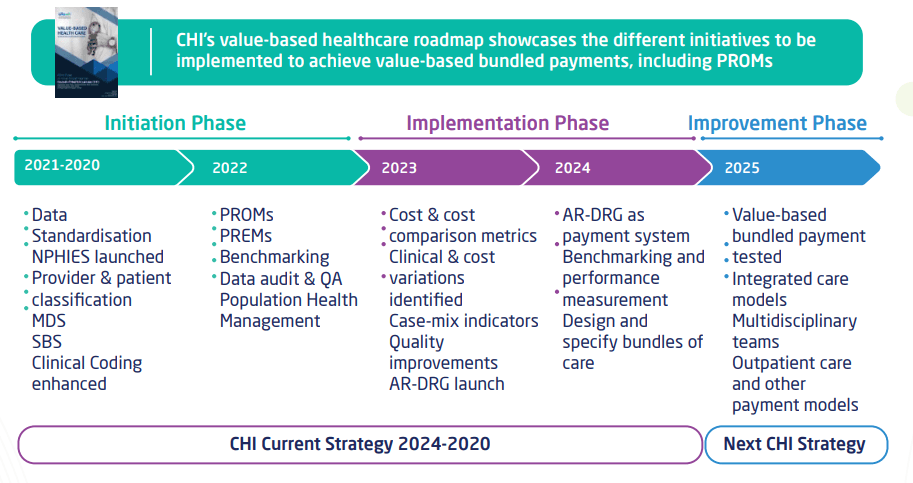
The CHI presented their roadmap on how they plan to introduce Value-Based payment models. The proposed approach will be implemented in four phases, where certain pre-requisites are required to progress to the next stage. All phases have prior dependencies on different pre-requisites and their delivery is conditional in achieving the final goal.
Saudi Billing System
The first step that CHI has taken was to introduce a billing system known as Saudi Billing System (‘SBS’) to standardize payments in the scheme. As a result, all CHI participants use the same set of codes.
AR-DRG System
The next step is to shift to a case payment model for admitted care services. As Saudi Arabia has subscribed to ICD-10 AM/AR-DRG system, it is expected that in Phase 2 and 3, CHI will introduce this system as a main reimbursement model for inpatient services. However, there are certain per-requisites to achieve this shift to case payment. Some of the main pre-requisites will be accurate clinical documentation and accurate and complete coding of inpatient episodes, estimation, or actual calculation of AR-DRG relative resource weights for services rendered under CHI scheme.
Bundled payment services.
The CHI will define payment bundles for 7 select conditions/procedures and develop the pathway and design of the payment bundle based on market preparedness and cost analysis through claims data, and stakeholder consultations. Already shortlisted conditions/procedures under Value Based Payment Pilot Project include cataract surgery, diabetes, pregnancy and childbirth, bariatric surgery.
The project delivery is structured in four phases:
Derive learnings from best practices;
Claims data analysis;
Define clinical pathways and outcome measures; and
Develop payment bundle & implementation plan.
CHI has developed an action plan based on the commitments set out in its strategy:
CHI Action 1: Standardized Patient Reported Measure Program
CHI Action 2: Population Health Program
CHI action 3: Primary Care Program
CHI Action 4: Australian Refined Diagnosis Related Group (AR-DRG)
CHI Action 5: Market Reference Price Project (MRP)
CHI Action 6: Bundled Payments
CHI Action 7: Value Based Payment Program Pilot
In 2023, CHI issued version 2 of the SBS and the Saudi Billing System Coding Standards (‘SBSCS’), which was implemented on 1 June 2023 (‘SBS V2"’). SBS V2 includes additional codes to those in V1, including non-billable codes; take care not to miss these additional codes that are required to be coded.
However, while SBS V3 is not officially launched yet, CHI is conducting workshops to a preview and deeper understanding of the expected new classifications and governance frameworks. This article focuses on V2 of 2023.
SBS V2SBS V2 (which includes SBS and SBSCS updates) updates and replaces the previously released "Standards and Guidelines of CCHI Billing System" of July 2020, and must be used in conjunction with the Australian Consortium for Classification Development (2017) Australian Coding Standards (‘ACS’) (both standards are to be reviewed together). Thus, this updated document should be used in conjunction with ACS 10th Edition.
The SBS is a modification to the Australian Classification of Health Interventions (‘ACHI’). According to CHI, the purpose of the SBS is to standardise data for claims, and for morbidity analysis and mandated reporting. CHI states that the SBS enables the translation of diagnoses and procedures and other health problems from words into an alphanumeric/numeric code, which permits easy storage, retrieval and analysis and use of the data.
Specifically, CHI reports that the ACHI codes have been modified for Saudi Arabia to allow inclusion of additional codes (including laboratory and pathology, ambulance and transport services, service codes or billing services) and further splits on unilateral/ bilateral procedures. SBS retains the same core 7-digit code as ACHI and includes two-digit extensions where greater specificity has been added to an ACHI code, including laterality.
The term 'clinician' is used throughout the document and refers to the treating physician but may also refer to midwives, nurses and allied health professionals
SBS V2 includes the following key updates:
SBS
765 new SBS codes;
1,531 revised descriptions;
132 deleted (inactivated) SBS codes;
2 new chapters (including Emergency Medical Services and Mortuary Services); and
4 new blocks.
SBSCS62 new standards (including General standards, Dental Services Imaging Services, KSA Services, Emergency Medical Services, Ambulance and Mortuary Services chapters).
SBS BackgroundThe private health insurance market in Saudi Arabia is regulated by the CHI. To support the market, one of CHI's strategic aims is to provide a standardized code set for billing interventions that providers submit to health insurers. The following healthcare services rendered in an ambulatory, secondary, or tertiary environment should be coded and billed:
Outpatient Medical Services;
Admitted Care Medical Services;
Consultation & Rounding Services;
Dental Services;
Laboratory & Pathology Services;
Radiology and Imaging Services;
Ambulance & Transportation Services;
Mortuary Services;
Emergency Medical Services (EMS); and
Room & Board.
SBS adapts Australian systems for Saudi healthcare, with new codes for outpatient, EMS, and home health services.
The SBSCS are based on the ACS for the International Statistical Classification of Diseases and Related Health Problems, Tenth Revision, Australian Modification (‘ICD-10- AM’) and ACHI, both 10th Edition.
The SBS includes the following classification standards:
ICD-10-AM;
SBS procedure codes;
SBSCS;
ACS;
the SFDA -GTIN - for Medications and Herbals/Vitamins; and
the SFDA -GMDN -for Medical Devices and Consumables.
As of 1 January 2020, Saudi Arabia has mandated the 10th Edition of ICD-10-AM/ACHI/ACS. SBS is built on the Australian systems, specifically ICD-10-AM and ACHI, but differs from the Australian system in two fundamental ways, as reported by CHI:
"Many new codes have been added (for example, for laboratory, evaluation and management-type interventions, emergency services, laboratory and pathology, and mortuary), more extensive unilateral and bilateral splits and the code structure has been modified from ACHI;
SBS is intended for both admitted and non-admitted care, unlike ACHI. Non-admitted care includes hospital outpatient visits, office-based specialist physician visits, emergency department visits, home health care and primary care".
These updates reflect the commitment of the sector to the objectives of the health sector transformation under Saudi Vision 2030. Health sector transformation in the Kingdom is not an incremental amendment but rather represents a shift in the fundamental concept of healthcare to the modern healthcare model – value based healthcare. This model focuses on enhancing prevention before treatment, contributing to the provision of comprehensive healthcare, raising awareness, and facilitating access to healthcare services for all citizens, towards achieving good health and well-being of nation.
For further information,please contact healthcare@tamimi.com.
Published in January 2025